You may be reading this because something looks off when you or your child bites down. Maybe the top teeth tuck behind the bottom teeth in one spot. Maybe your child shifts their jaw to one side to get their teeth to fit. Maybe you've been told you have a crossbite and you're wondering whether this is a cosmetic issue, a functional issue, or both.
I'm Dr. Finley, and many patients in Santa Ana and nearby Orange County communities start here. They want a clear explanation, not jargon. They want to know whether it's safe to watch and wait, when treatment matters, and what realistic options exist for children, teens, and adults.
Table of Contents
- What Is a Crossbite and Why Does It Matter
- Common Causes and How We Diagnose a Crossbite
- Early Crossbite Treatment for Children
- Modern Crossbite Solutions for Teens and Adults
- Your Treatment Journey and Long-Term Success
- Understanding Surgical Options for Severe Crossbites
- Your Next Step Toward a Healthier Bite
What Is a Crossbite and Why Does It Matter
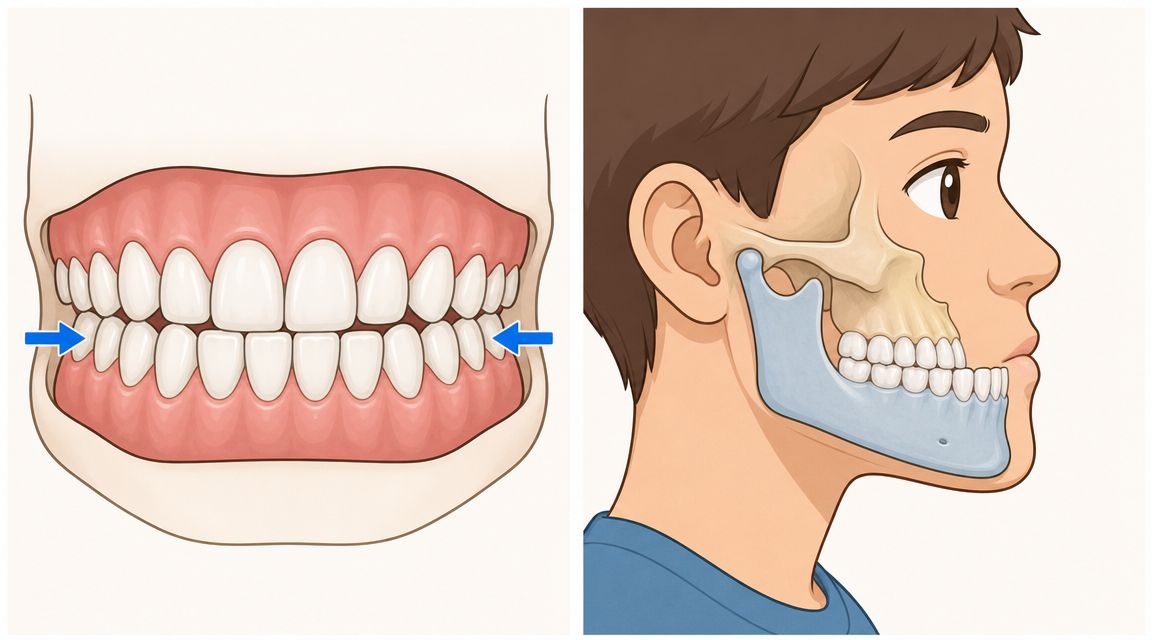
A crossbite means some upper teeth bite inside the lower teeth instead of outside them. A simple way to picture it is a lid that doesn't sit properly on a box. The parts may look close, but they don't fit the way they were designed to.
That matters because your bite is a working system. Teeth guide chewing. The jaw closes in a repeatable path. Muscles adapt to the way the teeth meet. When one part is out of position, other parts often compensate.

Two common types
| Type | What it means in plain language | What people often notice |
|---|---|---|
| Anterior crossbite | One or more front upper teeth sit behind the lower front teeth | The front teeth look reversed or edge-to-edge |
| Posterior crossbite | Upper back teeth bite inside the lower back teeth | One side may feel “off,” narrow, or shifted |
Some crossbites involve just one tooth. Others involve several teeth or the way the upper and lower jaws relate to each other.
Why dentists pay attention to it
A crossbite isn't only about appearance. It can affect how forces are distributed when you chew. Over time, that may contribute to uneven tooth wear, irritation around certain teeth, and strain on the bite.
Children can also develop a habit of sliding the jaw to one side to avoid a bite interference. When that happens early and repeatedly, we pay attention because growth tends to follow function. Adults usually describe the problem differently. They often say one side hits first, chewing feels unbalanced, or one tooth seems to take too much pressure.
Practical rule: If the bite looks shifted, feels forced, or closes differently from one side to the other, it's worth having it evaluated.
People also get confused about whether every crossbite needs immediate care. The answer is no. Some situations can be monitored for a period of time, especially if we're waiting for more teeth to erupt or confirming whether the bite issue is developing. But watchful waiting should be intentional, not accidental. It should follow an exam, not guesswork.
That's the key idea behind crossbite treatment. We aren't just trying to “straighten teeth.” We're trying to create a bite that fits together more naturally and functions with less strain.
Common Causes and How We Diagnose a Crossbite
Crossbites don't come from one single cause. Sometimes the upper jaw is narrow because of growth pattern and family traits. Sometimes a child develops a bite issue after habits like thumb sucking or long-term pacifier use. In other cases, teeth erupt into a crowded or blocked position and end up biting the wrong way.
Adults can carry a childhood crossbite into later life, or they may notice the problem more after teeth shift, restorations change the bite, or crowding becomes more obvious.
Causes we commonly look for
- Genetic jaw pattern can make the upper arch narrower or change how the upper and lower jaws relate.
- Oral habits may influence tooth position and arch shape during development.
- Eruption problems happen when incoming adult teeth don't have a clear path.
- Premature tooth loss or crowding can redirect where neighboring teeth settle.
A diagnosis starts with something simple. We watch how you close. Not how you think you close, but how your teeth meet when your jaw relaxes into place. That tells us whether the problem is a single tooth, a whole segment of teeth, or the jaw relationship itself.
What the exam usually involves
At a visit, we typically combine several pieces of information:
- Visual bite exam to see where the teeth contact and whether the jaw shifts.
- Digital X-rays to check roots, eruption pattern, and supporting structures.
- 3D intraoral scanning to create a detailed model of the bite without messy impressions.
A good treatment plan starts with the right diagnosis. A narrow upper arch, a tipped tooth, and a jaw-position problem can all look similar at first glance, but they are not treated the same way.
That distinction is where people often feel relieved. Once we identify whether the crossbite is mostly dental or more skeletal, the next step becomes much easier to understand. A dental problem often means tooth movement can solve it. A skeletal problem means we also have to think about the shape or width of the jaw, especially in growing children and in adults whose growth is complete.
Early Crossbite Treatment for Children
Children give us an opportunity adults no longer have. Their jaws are still developing. That means crossbite treatment can often guide growth instead of fighting against a fully finished skeletal pattern.
For parents, this is usually the central question. Should we act now, or can we wait?
When early treatment makes sense
Early treatment is often worth considering when a child:
- Shifts the jaw to one side to make the teeth fit
- Shows a narrow upper arch with back teeth biting inside
- Has a front tooth trapped behind the lower teeth
- Looks uneven when biting down, even if only one area seems affected
When I recommend early care, it's usually because the bite is affecting function, not because I'm trying to rush a child into orthodontics. Some children need active correction. Others need monitoring until the timing is better.

Why timing matters in growing patients
Posterior crossbite is common in young patients, with prevalence estimates of about 17% in America among children and adolescents, according to a Cochrane review on posterior crossbite treatment in growing patients. That same review found that interceptive treatment can create measurable widening of the upper arch. For example, a Hyrax expander increased intermolar width by an average of 5.80 mm in adolescents, and the review included 31 trials overall.
Those numbers matter because they show why early treatment is more than a cosmetic conversation. In the right child, an appliance can create real space and improve the way the upper and lower arches fit together.
What these appliances do
A palatal expander is designed to gently widen the upper arch over time. Parents sometimes picture something dramatic, but the concept is straightforward. If the upper jaw is too narrow for the lower teeth to fit under it properly, we create room where room is missing.
Common early tools may include:
- Expanders when the upper arch needs width
- Fixed braces on selected teeth when a single tooth needs controlled movement
- Removable appliances in mild, well-selected cases
Early treatment doesn't always mean full braces for years. Sometimes it means a focused first phase that solves one important problem at the right time.
Watchful waiting can still be the right choice in some children. If the bite is borderline, if adult teeth are still erupting, or if there's no functional shift, we may monitor. But if the child is biting into an unstable pattern, using growth sooner can be much simpler than trying to correct the same skeletal mismatch later.
For families in Santa Ana, Tustin, Costa Mesa, Irvine, and Garden Grove, that's often the biggest benefit of an early orthodontic evaluation. You get a roadmap. Sometimes the answer is “treat now.” Sometimes it's “not yet, but here's what we're watching.”
Modern Crossbite Solutions for Teens and Adults
A teen may sit in the chair with a crossbite that is partly dental and partly tied to jaw growth. An adult often asks a different question. Can this be fixed without surgery?
Those are not the same treatment conversation.
Once growth is further along, we spend less time trying to guide the jaws and more time deciding what can be corrected by moving teeth, what can be improved by changing arch width in a limited way, and what may need surgical support if the jaw position is the main issue. The key first step is sorting out whether the crossbite is mostly dental or skeletal.
A dental crossbite means the teeth are out of position, even if the upper and lower jaws are fairly compatible. A skeletal crossbite means the jaw relationship itself is part of the problem. That difference matters because teeth can be moved within bone, but tooth movement alone cannot fully reshape an adult jaw.
Braces, clear aligners, and other non-surgical options
For teens and adults with a dental crossbite, non-surgical treatment is often the starting point. The appliance is just the tool. What matters more is which tool gives the type of control your bite needs.
| Option | Often useful for | Main strength | Main limitation |
|---|---|---|---|
| Braces | Many dental crossbites and complex tooth movements | Strong control over tooth roots and crowns | More visible |
| Clear aligners | Mild to moderate dental crossbites in selected cases | Appearance and removability | Not ideal for every movement pattern |
| Removable expander at night | Mild adult crossbite in selected cases | Non-surgical option for limited situations | Not appropriate for severe skeletal problems |
Clear aligners can work well in selected cases, especially when the problem is mostly tooth position. Braces often give us more precise control when the bite is more complex or when roots need careful repositioning, not just the visible part of the tooth. A removable nighttime expander may help in limited adult cases, but it is not a substitute for correcting a larger jaw mismatch.
That last point is where confusion often starts. Patients hear that an appliance can "expand" and assume all expansion means the same thing. It does not. In a growing child, expansion can influence a developing upper jaw. In an adult, non-surgical expansion is usually more limited and often involves tooth movement rather than a true skeletal change.
A realistic way to think about teen treatment
Teens sit in the middle. Some still have growth left. Some are already close to an adult pattern.
That is why a teenager with a crossbite may have more options than an adult, but fewer than a younger child. If there is useful growth remaining, treatment may be able to combine bite correction with some orthopedic benefit. If growth is nearly complete, the plan starts to look much more like adult treatment, with a stronger focus on tooth movement and realistic limits.
For parents, this is often the most helpful message. A teen evaluation is not just about asking, "Do they need braces?" It is about asking, "Are we still in a window where growth helps us, or are we mainly correcting tooth position now?"
Why single-tooth crossbites still need careful planning
A crossbite involving one tooth can look minor in the mirror and still need precise mechanics. According to StatPearls guidance on posterior crossbite management, 3/16-inch cross-elastics delivering about 2.5 to 4.5 oz of force can help correct selected posterior single-tooth crossbites.
That detail matters because correcting a crossbite is not just about pushing a tooth outward. The tooth has to land in a stable position where the top and bottom teeth meet evenly. If the force is poorly directed, the crown may tip while the root stays in a less stable position. Fixed appliances often help us control that movement more accurately in three dimensions.
A good way to picture it is straightening a fence post. If you only push the top, it may look better for a while, but the base is still off.
Bristol Dental & Orthodontics provides orthodontic care for crossbites in teens and adults, including braces, clear aligner therapy, and other bite-correction options. The right plan depends on the diagnosis, not on which appliance sounds simplest.
For adults, the most honest answer is often the most reassuring one. Many mild to moderate crossbites can be improved without surgery when the problem is mainly dental. If the crossbite is severe and skeletal, non-surgical treatment may improve appearance and function to a degree, but it may not fully correct the underlying jaw relationship.
Your Treatment Journey and Long-Term Success
Patients often want to know two things after diagnosis. What happens first, and how do I keep the result from slipping back?
The first part is straightforward. We confirm the type of crossbite, choose the appliance that matches it, and move in stages. Some patients begin with expansion. Others start with alignment. Some need both, but not at the same time.
The usual sequence
- Evaluation and records establish exactly what needs correction.
- Active treatment addresses the crossbite using the chosen appliance.
- Finishing phase refines contacts so the bite fits more evenly.
- Retention holds the result while teeth and supporting tissues adapt.
Treatment length depends on complexity, age, cooperation, and whether the issue is isolated to one area or tied to a broader bite pattern. That's why it's hard to give a meaningful timeline before an exam.
Why retention is not optional
This is the part patients sometimes underestimate. Teeth have memory, and the surrounding tissues need time to stabilize after movement. Long-term evidence shows that relapse is a real part of crossbite care if retention is ignored.
A meta-analysis found that about 1 in 5 patients may experience some relapse after correction, which is why long-term retention after posterior crossbite correction matters. In plain terms, the retainer isn't a small add-on. It protects the work you just completed.
If active treatment builds the result, retention protects it.
Patients also ask about cost. The honest answer is that cost depends on the appliance, the complexity of the bite, whether treatment is limited or extensive, and whether other procedures are involved. A personalized exam is the right place for that discussion because the fee should match the actual plan, not a generic number from the internet.
Understanding Surgical Options for Severe Crossbites
Surgery sounds intimidating to many adults, but the idea is often simpler than they expect. If the crossbite comes mainly from how the jaws are built and growth is complete, orthodontics alone may not be able to move the teeth into a healthy bite without compromising something else.
In those cases, orthognathic treatment combines braces or aligners with jaw surgery to place the jaws in a better relationship. The orthodontic part lines up the teeth. The surgical part addresses the skeletal mismatch that tooth movement alone can't fully solve.
When surgery enters the conversation
Surgical options are usually considered when:
- The problem is skeletal, not just dental
- The upper jaw is too narrow or the jaw relationship is more severe
- Camouflage treatment would leave the bite unstable or compromised
This isn't a first-line recommendation for every adult with a crossbite. It's a specific solution for specific anatomy.
What the process usually looks like
Care is collaborative. The orthodontist and oral surgeon plan the case together. Teeth are prepared orthodontically first, the surgical correction is performed, and then the bite is fine-tuned afterward.
Surgery is not a failure of braces or aligners. It's the right tool when the jaws, not just the teeth, need correction.
For many adults, the most reassuring part is hearing that there is a path forward. Some people are good candidates for non-surgical care. Others will get a more stable, functional result with combined treatment. The important thing is knowing which group you're in before starting.
Your Next Step Toward a Healthier Bite
A parent often comes in asking one simple question: “Do we need to do something now, or can we safely wait?” Adults usually ask a different version of the same concern: “Is there still a realistic fix for me?” Those are the right questions.
Crossbite treatment is not one-size-fits-all. A child with a small bite interference may need monitoring while the mouth develops. Another child may need early treatment because the bite is guiding the jaw into the wrong path, like a door that keeps closing into an off-center frame. For adults, the decision usually comes down to whether the problem is mainly in the teeth, mainly in the jaws, or a mix of both.
Does crossbite treatment hurt
Most children, teens, and adults describe treatment as pressure or soreness, especially after an appliance is placed or adjusted. That feeling is usually temporary. Soft foods, a little patience, and good home care make the adjustment period easier.
Can a crossbite get worse if I leave it alone
Sometimes yes. Some cases change slowly, but others lead to uneven tooth wear, shifting, gum strain, or a bite that becomes more difficult to correct later. In a growing child, the bigger concern is whether the bite is pushing the jaw to close in an unhealthy pattern. That is one of the main reasons an exam matters.
Am I too old for treatment
No.
Adults can often improve a crossbite with braces or clear aligner therapy, depending on the type and severity of the problem. Age matters less than diagnosis. What matters is whether the teeth can be moved into a stable position without asking them to compensate for a jaw problem they cannot fix on their own.
Why does this matter for other dental work
Your bite works like the foundation under a house. If the foundation is off, cosmetic work, tooth replacement, and even routine restorations have to absorb forces they were not designed to handle. A healthier bite helps natural teeth and dental work function more evenly over time.
If you live in Santa Ana, Costa Mesa, Tustin, Irvine, Garden Grove, or nearby Orange County, the next step is simple. Get an exam that answers three questions clearly: what kind of crossbite you have, whether this is a watch-and-monitor situation or a treat-now situation, and which options are realistic for your goals and age.
If you'd like personalized guidance, schedule a consultation with Bristol Dental and Orthodontics. We'll evaluate the bite, explain whether watchful waiting or active crossbite treatment makes sense, and help you understand the options for your specific case.